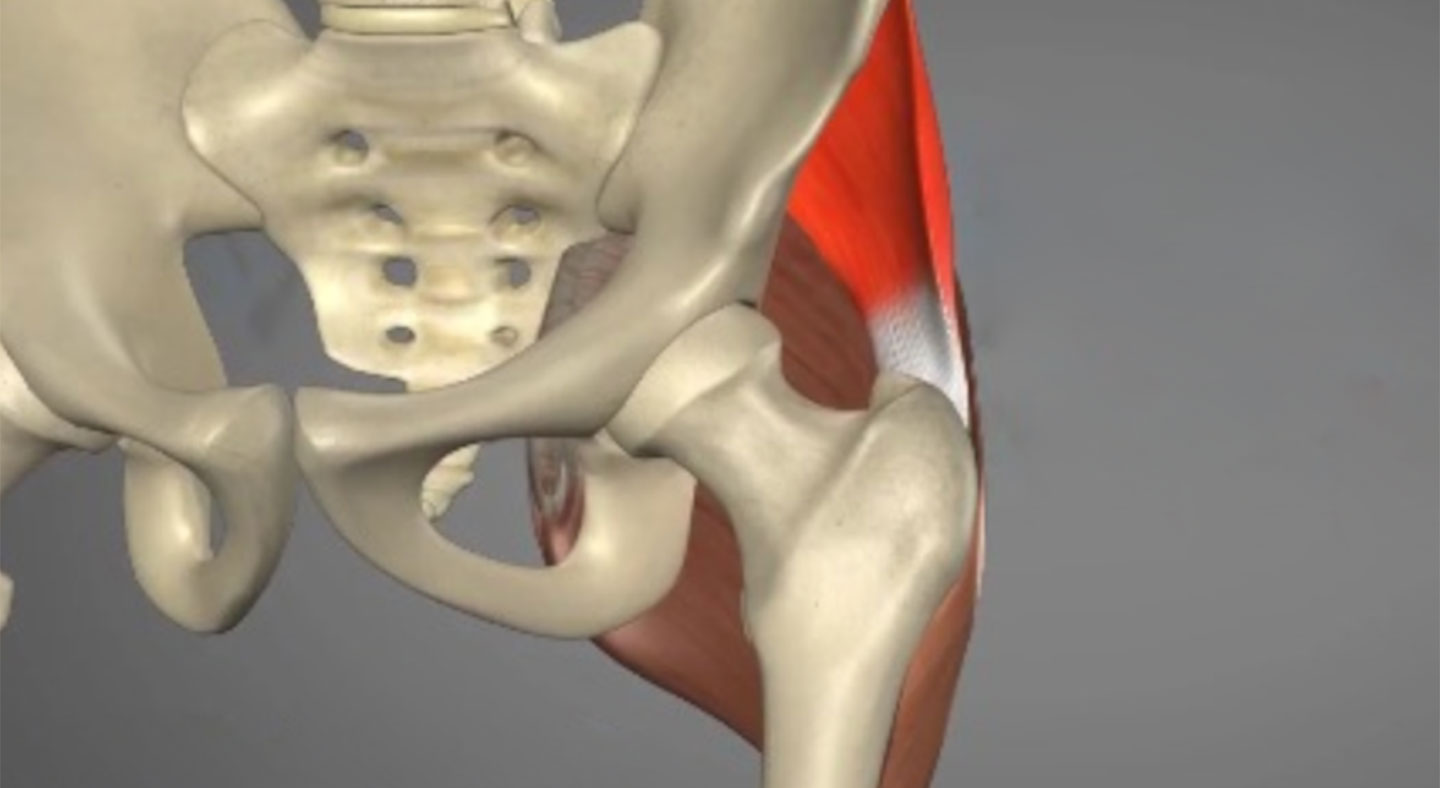
The hip abductors (comprising the gluteus medius and gluteus minimus muscles) are often referred to as the “rotator cuff” of the hip. They function to abduct the hip and also to stabilize the pelvis while in single-leg stance (during running, jumping, pivoting, cutting or when going up and down the stairs…).
Hip abductor tendon injuries or tears are diagnosed by combining clinical symptoms (pain, weakness) with MRI findings indicative of tendon degeneration, partial thickness tearing, or complete tearing.
Hip abductor tendon injuries are different from muscle injuries, and are divided into two types: acute and chronic.