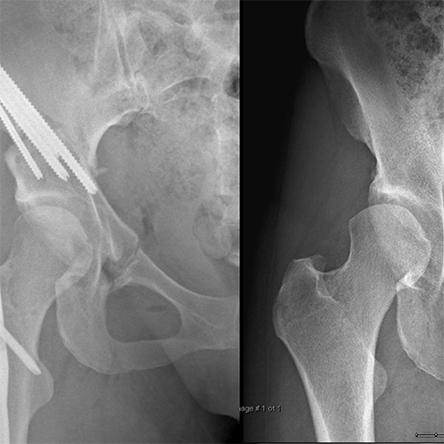
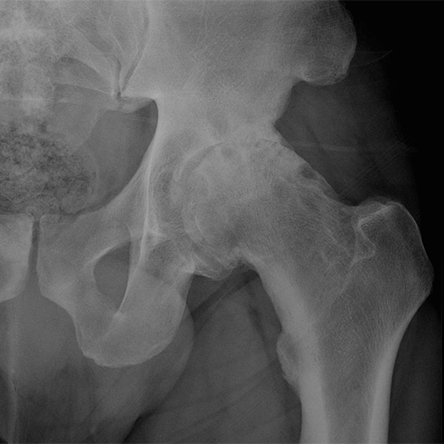
Arthritis is diagnosed by combining clinical symptoms (pain, stiffness, swelling, deformity) with radiographic (x-ray) findings (joint space loss, bone spur formation, cysts). Occasionally, patients will present with radiographic evidence of arthritis and have minimal clinical symptoms. Even if the x-rays show “bone-on-bone” arthritis, the treatment is always guided by the clinical symptoms and not the radiographic findings.